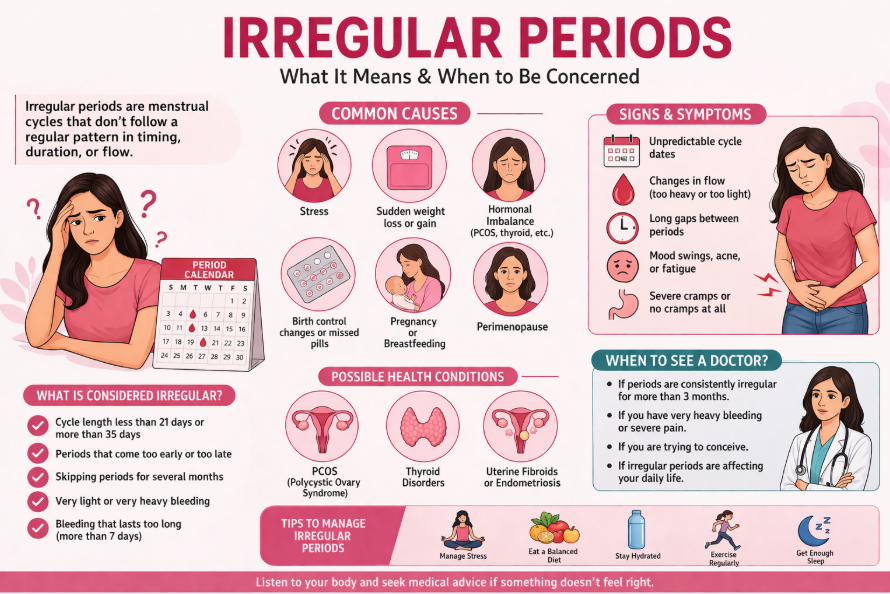
An irregular period is one of the most common reasons people search for a gynaecologist because it can be confusing, inconvenient, and sometimes scary. One month your period arrives early, the next month it’s late, or the bleeding pattern changes completely. The important thing to know is that irregular cycles can happen for many reasons, some harmless and temporary (like stress or early puberty), and others that deserve medical attention (like PCOS, thyroid problems, fibroids, or endometriosis).
Irregular cycles are also not rare: the NICHD estimates 14% to 25% of women have irregular menstrual cycles.
This article explains what counts as an irregular period, the most common causes, how doctors diagnose it, and the red flags that tell you when to worry.
Medical note: This is general health information, not a diagnosis. If you’re bleeding heavily, feeling faint, or have severe pain, seek urgent medical care.
Irregular period meaning: what’s normal vs. irregular
Before calling something an irregular period, it helps to know what “regular” means.
What’s considered a normal cycle?
For many adults, menstrual bleeding happens about every 28 days, but normal ranges are wider:
- Cycle interval often ranges from 21 to 35 days
- Bleeding commonly lasts 2 to 7 days
What’s considered an irregular period?
An irregular period can include:
- cycles shorter than 21 days or longer than 35 days (adults)
- a pattern that keeps changing significantly month-to-month
- missing 3 or more periods in a row (in some contexts)
- bleeding that is much heavier, lighter, or longer than your usual pattern
What about teens and first periods?
In adolescents, irregularity can be common early on. ACOG notes that by the third year after the first period, most cycles become more adult-like: 60–80% fall between 21–34 days.
ACOG also highlights that many teens have cycles 21–45 days and bleeding typically ≤7 days.
Irregular period patterns (missed, frequent, heavy, spotting)
Irregular periods don’t look the same for everyone. Identifying your pattern helps narrow down causes.
Irregular period pattern 1: Missed or very infrequent periods (oligomenorrhea/amenorrhea)
Common clues:
- long gaps (e.g., 45–60+ days)
- no period for 3 months or more
Potential links: stress, significant weight change, PCOS, thyroid issues, elevated prolactin, premature ovarian insufficiency (less common).
Irregular period pattern 2: Frequent periods (polymenorrhea)
Common clues:
- cycles shorter than 21 days repeatedly
Potential links: hormonal imbalance, thyroid issues, perimenopause, some uterine conditions.
Irregular period pattern 3: Heavy or prolonged bleeding
Heavy bleeding is common enough that about one third of women seek treatment for it, according to ACOG.
Heavy bleeding can raise the risk of iron deficiency anemia over time, which is why persistent heavy periods shouldn’t be brushed off.
Irregular period pattern 4: Spotting between periods or after sex
Bleeding between periods or after sex can be due to several causes, from infections to cervical issues; this is one of the patterns where you should book an evaluation rather than wait.
Irregular period causes: the most common reasons
Many irregular periods come from the same core issue: ovulation isn’t happening regularly (anovulation), or the uterine lining is being affected by hormones, inflammation, or structural changes.
Irregular period causes: a data snapshot (why this topic is so common)
| Condition linked to irregular periods | What the data says | Why it matters |
| Menstrual irregularities overall | 14–25% have irregular cycles (NICHD) | Common, but needs context |
| PCOS | Affects ~10–13% of reproductive-aged women (WHO) | A leading cause of irregular ovulation |
| Endometriosis | Affects ~10% (190 million) globally (WHO) | Can cause painful/heavy periods |
| Uterine fibroids | Estimated 20–40% in reproductive age (NCBI Bookshelf/StatPearls) | Can cause heavy or irregular bleeding |
| Bleeding disorders (relevant in teens with heavy bleeding) | General population ~1–2%, but found in ~20% of adolescents with heavy menstrual bleeding (ACOG) | Important “missed cause” in teens |
1) Stress, sleep disruption, and major life changes
Stress affects hormones that regulate ovulation. Big exams, family stress, travel, illness, or major sleep changes can shift cycles temporarily.
Tip: If irregularity starts during a stressful period and improves when life stabilizes, stress may be a major contributor but still track it.
2) Weight change, under-eating, or intense exercise
Rapid weight loss, restrictive dieting, or intense training can reduce signals from the brain to the ovaries, leading to infrequent or missed periods. (This is especially relevant in teens and athletes.)
3) Polycystic ovary syndrome (PCOS)
PCOS is one of the most common hormonal reasons for an irregular period. WHO estimates PCOS affects 10–13% of reproductive-aged women, and notes that up to 70% may be undiagnosed.
Common signs that can appear with irregular periods
- acne or increased hair growth (not always)
- weight changes (not always)
- difficulty predicting ovulation
PCOS care is increasingly guided by international evidence-based recommendations (ASRM hosts the 2023 guideline summary).
4) Thyroid disorders (hypothyroid or hyperthyroid)
Thyroid hormones influence menstrual regularity. Clinical reviews note thyroid dysfunction is commonly seen in people presenting with abnormal uterine bleeding.
Clues you might notice
- fatigue, weight change, constipation, temperature sensitivity, hair changes
(These symptoms are not specific—testing is the only way to know.)
5) Endometriosis
Endometriosis affects about 10% (190 million) reproductive-age women globally, per WHO.
It’s classically linked to significant period pain, but can also involve heavy bleeding and ongoing pelvic discomfort.
6) Uterine fibroids (leiomyomas)
Fibroids are common benign growths in the uterus. Estimates vary, but one clinical review notes 20–40% prevalence in reproductive-age women.
Fibroids can contribute to heavy or irregular bleeding and pressure symptoms.
7) Contraception changes (or missed doses)
Starting, stopping, or switching hormonal contraception can cause breakthrough bleeding or cycle changes. Missing pills can also trigger irregular bleeding patterns.
8) Perimenopause (the transition before menopause)
As the ovaries shift in hormone production, cycles often become irregular. NHS notes irregular periods are common near menopause.
(If you’re 40+ and cycle changes are new, it’s still worth evaluating don’t assume it’s “just age.”)
9) Pregnancy (including early pregnancy bleeding)
If pregnancy is possible, it must be ruled out when bleeding is abnormal clinical guidance emphasizes pregnancy testing in reproductive-age patients with abnormal bleeding.
Irregular period diagnosis: how doctors find the cause
A good evaluation doesn’t just “stop the bleeding.” It identifies why your period became irregular and checks for complications like anemia.
Step 1: History (your story matters)
Expect questions about:
- cycle length and date of last period
- how heavy bleeding is (pads/tampons per day)
- bleeding between periods or after sex
- pain pattern (during periods vs. all month)
- recent stress, weight changes, new exercise routines
- medications, contraception, and supplements
- family history (thyroid disease, bleeding disorders)
Step 2: Physical exam (when appropriate)
Depending on age and symptoms, a clinician may do:
- general exam (thyroid signs, acne, body hair pattern)
- abdominal/pelvic exam (when clinically appropriate)
Step 3: Key tests for an irregular period
A commonly referenced approach to abnormal uterine bleeding includes labs such as pregnancy test, TSH, and prolactin, with further testing based on risk factors.
Table: Common tests and what they look for
| Test | Why it’s ordered | What it can help identify |
| Pregnancy test | Rule out pregnancy-related bleeding | Pregnancy, early complications |
| CBC (blood count) | Check anemia | Low hemoglobin from heavy bleeding |
| Ferritin / iron studies | Assess iron stores | Iron deficiency from long-term heavy periods |
| TSH | Check thyroid function | Hypo/hyperthyroidism linked to bleeding changes |
| Prolactin | Check prolactin level | Elevated prolactin can disrupt ovulation |
| Pelvic ultrasound | Look at uterus/ovaries | Fibroids, cysts, structural causes |
| Additional hormone tests (case-by-case) | Evaluate ovulation/ovarian reserve | PCOS patterns, other endocrine issues |
Special consideration: teens with heavy bleeding
If a teen has heavy bleeding, clinicians may consider bleeding disorders. ACOG notes bleeding disorders occur in ~20% of adolescents presenting with heavy menstrual bleeding.

Irregular period: when to worry (red flags)
Some symptoms suggest you shouldn’t wait months to “see if it settles.”
Seek urgent care (same day) if you have:
- very heavy bleeding with dizziness/fainting
- severe pain with vomiting or weakness
- signs of significant anemia (shortness of breath, chest pain, fainting)
- possible pregnancy plus bleeding (especially with one-sided pain)
Book a medical appointment soon if you notice:
ACOG and NHS-style patient guidance highlights several “don’t ignore” patterns, especially heavy bleeding that affects life, severe pain, and bleeding between periods or after sex.
Table: Red flags and what they could mean
| Red flag symptom | Why it matters | Don’t self-diagnose get checked for… |
| Bleeding between periods | Not typical for many people | Hormonal issues, infection, polyps, cervical causes |
| Bleeding after sex | Needs evaluation | Cervical inflammation, infection, other causes |
| Periods suddenly much heavier | Risk of anemia + underlying causes | Fibroids, bleeding disorders, hormonal imbalance |
| Cycle gaps >90 days (especially teens) | Outside typical pattern | Ovulation disorders, endocrine causes |
| Severe period pain that disrupts life | Not “just normal cramps” | Endometriosis, other pelvic causes |
| Persistent irregularity >3 months | Needs systematic evaluation | PCOS, thyroid, structural causes |
Treatment options and what usually helps
Treatment depends on the cause, your age, and whether pregnancy is a current goal. Many plans combine symptom relief with long-term health protection.
1) Lifestyle supports (when appropriate)
Helpful when irregularity is linked to stress, sleep, sudden weight change, or overtraining:
- consistent meals and adequate nutrition
- balanced exercise (not extreme spikes)
- sleep routines
- stress management tools (support systems, counseling, relaxation)
2) Treat the underlying condition
Examples:
- PCOS: may include cycle regulation strategies and metabolic health support; care is guided by international evidence-based recommendations.
- Thyroid disorders: treating thyroid imbalance often improves cycles.
- Fibroids: management varies by size/symptoms; ultrasound helps guide options.
- Endometriosis: symptom control and evaluation plans may be needed.
3) Heavy bleeding-specific options (overview)
NICE provides evidence-based guidance for assessing and managing heavy menstrual bleeding with a focus on quality of life and cause-based treatment.
(Your clinician may discuss non-hormonal and hormonal options depending on your situation.)
Safety note: Do not start or stop prescription hormones without guidance especially if you have a migraine with aura, clotting history, or other risk factors.
4) Treat anemia if present
If heavy bleeding has caused iron deficiency, your clinician may recommend iron treatment and monitoring. WHO highlights anemia as a significant health issue for women of reproductive age.
How to track your cycle (and what to record)
Tracking turns a confusing irregular period into useful data for diagnosis.
What to record (simple checklist)
- first day of bleeding (Day 1)
- total days of bleeding
- heaviness (light/medium/heavy; how often you change pads)
- pain level (0–10)
- spotting between periods
- any new symptoms: acne, hair changes, weight changes, fatigue
- major stress/illness/travel
Table: A simple 3-month cycle tracker (copy/paste)
| Month | Day 1 date | Cycle length | Bleeding days | Heavy days? | Spotting between? | Pain (0–10) | Notes |
| Month 1 | |||||||
| Month 2 | |||||||
| Month 3 |
Bring this to your appointment—most clinicians will love you for it.
Choosing care locally (Kathmandu/Nepal)
If your irregular period is persistent, affecting your daily life, or paired with any red flags above, it’s reasonable to consult a gynaecologist in Nepal. If you’re based in the valley, you may look for a gynaecology clinic in Kathmandu with access to ultrasound and lab services for a complete evaluation.
Karuna City Clinic is a multispecialty clinic located in Naya Bazar, Kathmandu-16, and lists OB/GYN services among its departments.
(This article is informational; the best next step is a personalized medical assessment.)
FAQs
How common is an irregular period?
Irregular cycles are common. The NICHD estimates 14% to 25% of women experience irregular menstrual cycles.
What cycle length is considered irregular?
Many sources define irregularity as cycles occurring less than 21 days or more than 35 days apart for adults.
For teens, cycles can vary more early on; ACOG notes many teens have cycles 21–45 days.
Can stress cause an irregular period?
Yes, stress can disrupt the hormones that regulate ovulation. If stress is a contributor, cycles often improve when routines stabilize, but persistent irregularity should still be evaluated.
What is the most common hormonal cause of an irregular period?
PCOS is one of the most common causes of irregular ovulation and irregular periods; WHO estimates it affects 10–13% of reproductive-aged women.
When should I worry about an irregular period?
Worry less about a single “off” month and more about:
- heavy bleeding affecting daily life
- bleeding between periods or after sex
- severe pain
- cycle gaps >90 days (especially teens)
- symptoms of anemia (fatigue, dizziness)
- possible pregnancy plus bleeding